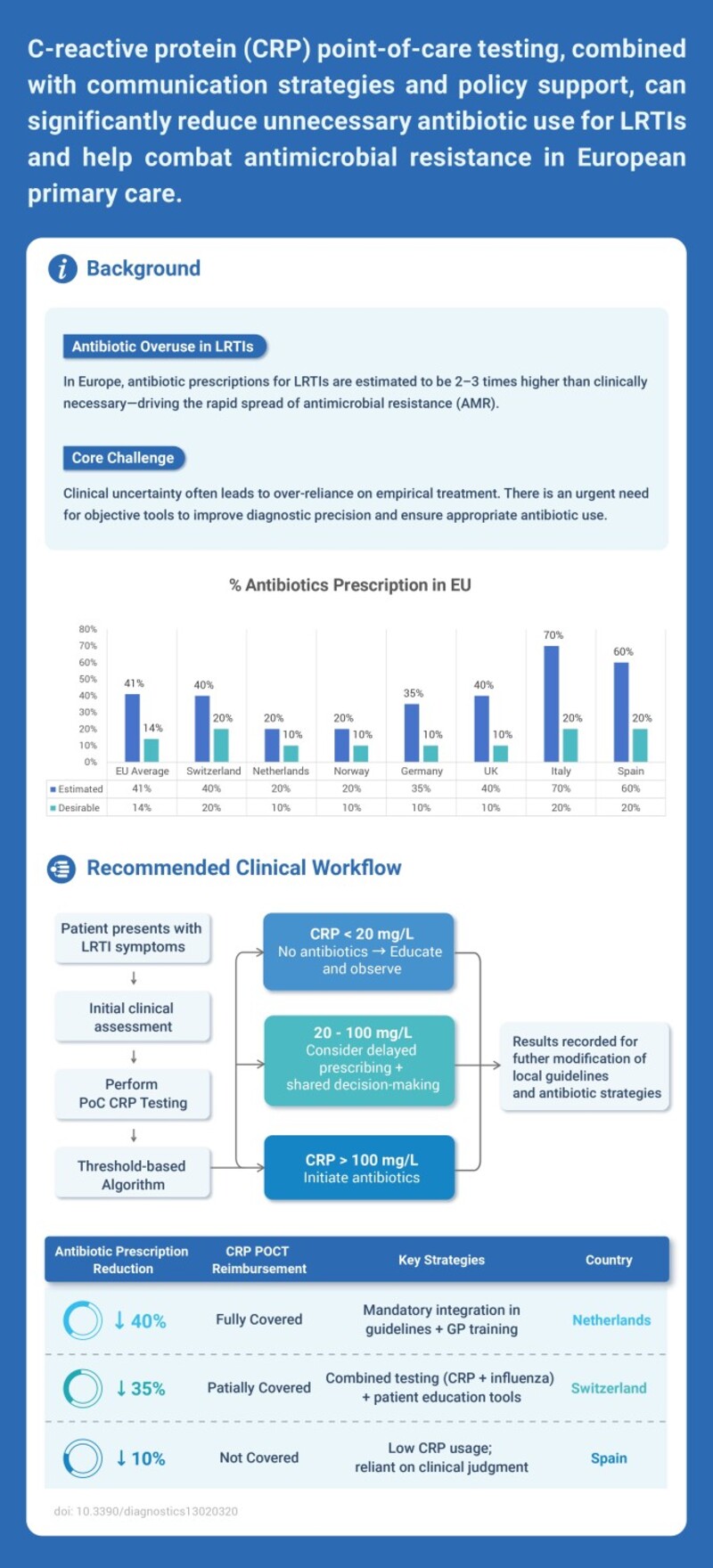
Antibiotic overuse in lower respiratory tract infections (LRTIs) remains a major driver of antimicrobial resistance (AMR), particularly in European primary care settings. Evidence suggests that C-reactive protein (CRP) point-of-care testing (POCT), when combined with effective communication strategies and supportive health policies, can significantly reduce unnecessary antibiotic prescribing.
Background: Antibiotic Overuse in LRTIs
In Europe, antibiotic prescriptions for LRTIs are estimated to be two to three times higher than clinically necessary. Diagnostic uncertainty often leads to empirical antibiotic use, highlighting the need for objective biomarkers to improve diagnostic precision and prescribing decisions.
Clinical Workflow for CRP-Guided Management
A structured CRP-based clinical workflow supports rational antibiotic use:
-
Patients presenting with LRTI symptoms undergo initial clinical assessment followed by CRP POCT.
-
CRP < 20 mg/L: Antibiotics are discouraged; patient education and observation are recommended.
-
CRP 20–100 mg/L: Delayed prescribing may be considered through shared decision-making.
-
CRP > 100 mg/L: Antibiotic treatment is initiated.
Test results can also inform future updates to local guidelines and antibiotic strategies.
Real-World Impact Across European Countries
Implementation outcomes vary across countries depending on reimbursement policies and guideline integration:
-
Netherlands: Full reimbursement and mandatory guideline integration resulted in approximately 40% reduction in antibiotic prescriptions.
-
Switzerland: Partial reimbursement combined with testing and patient education led to a 35% reduction.
-
Spain: Limited coverage and reliance on clinical judgment alone resulted in a smaller reduction of around 10%.
Conclusion
CRP POCT is an effective and accessible tool to reduce unnecessary antibiotic use in primary care. When supported by appropriate reimbursement policies, guideline integration, and clinician education, CRP testing plays a meaningful role in combating antimicrobial resistance.
Reference:
doi: 10.3390/diagnostics13020320



















 The first developed technology platform with various application scenarios, including infectious disease, fertility, DOA, etc.
The first developed technology platform with various application scenarios, including infectious disease, fertility, DOA, etc. 50+ kinds of reagents and five high-performance devices, focusing on detecting cardiovascular disease, inflammation, kidney injury, sex hormones, thyroid function, diabetes, tumor, and others.
50+ kinds of reagents and five high-performance devices, focusing on detecting cardiovascular disease, inflammation, kidney injury, sex hormones, thyroid function, diabetes, tumor, and others. Single-dose Chemiluminescense Immunoassay Platform
Single-dose Chemiluminescense Immunoassay Platform Wondfo optical blood coagulation analyzer is the first one in the world that can test PT, APTT, TT, FIB, and ACT simultaneously.
Wondfo optical blood coagulation analyzer is the first one in the world that can test PT, APTT, TT, FIB, and ACT simultaneously. Our Blood Gas Analyzer BGA-102 can produce the result in 30s. Its advantages of portability, easy operation, durability, and high performance make it ideal for clinics, laboratories, and hospitals.
Our Blood Gas Analyzer BGA-102 can produce the result in 30s. Its advantages of portability, easy operation, durability, and high performance make it ideal for clinics, laboratories, and hospitals. Ready-to-use lyophilized RT-PCR Reagent;
Ready-to-use lyophilized RT-PCR Reagent; Wondfo PA-3600 IHC Staining System
Wondfo PA-3600 IHC Staining System The Wondfo Truth-H80E HPLC Hemoglobin Analyzer is a high-performance diagnostic device designed for rapid and precise measurement of glycosylated hemoglobin (HbA1c)—the gold standard for diabetes diagnosis.It support the standard mode and variant mode and provide the result within 60-90seconds.
The Wondfo Truth-H80E HPLC Hemoglobin Analyzer is a high-performance diagnostic device designed for rapid and precise measurement of glycosylated hemoglobin (HbA1c)—the gold standard for diabetes diagnosis.It support the standard mode and variant mode and provide the result within 60-90seconds. Finecare™ Vitamin D, from complexity to simplicity
Finecare™ Vitamin D, from complexity to simplicity Building A World Free from Antibitoic Overuse
Building A World Free from Antibitoic Overuse Advanced rapid diagnostic test with WHO prequalification for infectious disease
Advanced rapid diagnostic test with WHO prequalification for infectious disease The Future Intelligent Medical Assistant to Healthcare
The Future Intelligent Medical Assistant to Healthcare Fight against the pandemic through continuous innovation
Fight against the pandemic through continuous innovation
















